
Morphological sub-classification of focal segmental glomerulosclerosis and their Clinio-pathological correlation: Experience from a tertiary care centre
Keywords:
FSGS, IgM nephropathy, Focal proliferative GN, Mesangioproliferative GN
Abstract
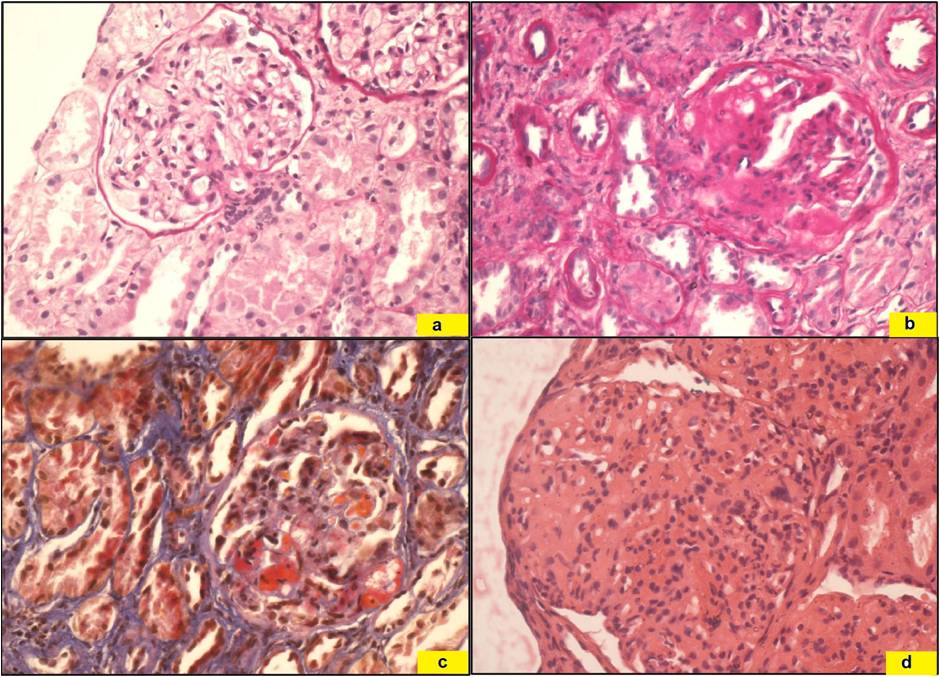
Background: The word focal segmental glomerulosclerosis (FSGS) is used to describe the common morphologic pattern occurring due to various progressive renal diseases and also to describe the primary idiopathic lesion of FSGS. Here, we are documenting the distribution of various types of FSGS and associated morphological lesion in the renal biopsy which may help to define the underlying cause of FSGSMethods: Total 47 cases of FSGS were retrieved from the archives and classified according to Agati’s classification. Acid Fuchsin Orange G (AFOG) stain was done to look for immune deposits. Direct immunofluorescence (DIF) was done in few cases.Result: FSGS - NOS was most common variant followed by perihilar and cellular variant. Focal segmental mesangial cell proliferation and GBM thickening were commonly found in NOS variant. Interstitial non caseating granulomas and mononuclear cell infiltrate admixed with neutrophils were more frequent in perihilar FSGS. Many cases earlier diagnosed as perihilar or tip lesion, latter turned out to be NOS variety on serial sections. AFOG stain revealed mesangial deposits in 70.22% cases, suggesting immunological aetiology of the disease instead of primary FSGS. DIF was performed in seven cases and all showed predominant IgM deposits in mesangium.Conclusion: Typing of FSGS should be done on the serial sections, especially of tip lesion. Most of FSGS cases turned out to be secondary to other glomerular disease instead of idiopathic variant. So, FSGS appear to be a morphological descriptor of various chronic renal diseases instead of being a separate entity.References
Beaufils H, Alphonse JC, Guedon J, Legrain M: Focal glomerulosclerosis: natural history and treatment. Report of 70 cases. Nephron. 1978; 21:75-85.
Magil AB: Focal and segmental glomerulosclerosis. Mod Pathol 1991; 4:383-391.
Mongeau JG, Robitaille PO, Glermont MJ, Merovani A, Russo P: Focal segmental glomerulosclerosis (FSG) 20 years later. From toddler to grown-up. Clin Nephrol. 1993; 40:1-6.
Nachmann PH, Jennett JC, Folk RJ: In Brenner and Rector’s: The kidney. Tal MW, Yu ASL, Chertow. 9th edition,Elsevier Saundus. 2012, 1111-1121.
D’Agati VD, Fogo A B, Bruijn JA, Jennette JC. Pathologic classification of focal segmental glomerulosclerosis: a working proposal.American journal of kidney diseases. 2004; 43(2):368-382.
Rennke H, Klein PS. Pathogenesis and significance of non primary focal and segmental glomerulosclerosis. Am J Kidney Dis 1989;13:443-55.
Franceschini N, North KE, Kopp J B, Mckenzie L, Winkler C. NPHS2 gene, nephrotic syndrome and focal segmental glomerulosclerosis: a HuGE review. Genetics in Medicine. 2006;8(2):63-75.
Koziell A, Grech V, Hussain S, Lee G, Lenkkeri U, Tryggvason K, Scambler P. Genotype/phenotype correlations of NPHS1 and NPHS2 mutations in nephrotic syndrome advocate a functional inter-relationship in glomerular filtration. Human Molecular Genetics.2002;11(4):379-388.
Weins A, Kenlan P, HerbertS, Le TC, Villegas I, Kaplan B S, Pollak M R. Mutational and biological analysis of α-actinin-4 in focal segmental glomerulosclerosis. Journal of the American Society of Nephrology.2005;16(12):3694-3701.
Winn MP, Conlon PJ, Lynn KL, Farrington MK, Creazzo T, Hawkins AF, Rosenberg PB. A mutation in the TRPC6 cation channel causes familial focal segmental glomerulosclerosis. Science. 2005;308:1801-1804.
Pollak MR. The genetic basis of FSGS and steroid-resistant nephrosis. In Seminars in nephrology. 2003; (Vol. 23, No. 2, pp. 141-146). WB Saunders.
Reiser J, Polu KR, Moller CC, Kenlan P, Altintas MM, Wei C, Pollak MR. TRPC6 is a glomerular slit diaphragm-associated channel required for normal renal function. Nature genetics,2005; 37: 739-44.
Hinkes B, Wiggins RC, Gbadegesin R, Vlangos CN, Seelow D, Nurnberg G, Hildebrandt F. Positional cloning uncovers mutations in PLCE1 responsible for a nephrotic syndrome variant that may be reversible. Nature genetics. 2006;38(12):1397-1405.
Diomedi-Camassei F, Di Giandomenico S, Santorelli FM, Caridi G, Piemonte F, Montini G, Emma, F. COQ2 nephropathy: a newly described inherited mitochondriopathy with primary renal involvement. Journal of the American Society of Nephrology. 2007;18(10): 2773-2780.
D'Agati V. Pathologic classification of focal segmental glomerulosclerosis. In Seminars in nephrology. 2003; (Vol. 23, No. 2, pp. 117-134). WB Saunders.
Zollinger HU, Mihatsch MJ: Renal Pathology in Biopsy: Light, Electron and Immunofluorescent Microscopy and Clinical Aspects. 1st edition. Springer Verlag Berlin Heidelberg New York. 1978:8-17.
Ferrario F, Rastaldi MP, Pasi A. Secondary focal and segmental glomerulosclerosis, Nephrology Dialysis Transplantation. 1999;14(SUPPL. 3):58-67.
Nada R, Kharbanda JK, Bhatti A, Minz RW, Sakhuja V, Joshi K. Primary focal segmental glomerulosclerosis in adults: is the Indian cohort different?.Nephrology Dialysis Transplantation.2009; 24(12): 3701-3707.
Das P, Sharma A, Gupta R, Agarwal SK, Bagga A, Dinda AK. Histomorphological classification of focal segmental glomerulosclerosis: A critical evaluation of clinical, histologic and morphometric features. Saudi Journal of Kidney Diseases and Transplantation.2012; 23(5):1008.
Shi SF, Wang SX, Zhang YK, Zhao MH, Zou WZ.Clinicopathologic study of different variants of focal segmental glomerulosclerosis. Chinese journal of pathology. 2007;36(1):11-14.
Silverstein DM, Craver R. Presenting features and short-term outcome according to pathologic variant in childhood primary focal segmental glomerulosclerosis. Clinical Journal of the American Society of Nephrology, 2007; 2(4): 700-707.
Stokes MB, Markowitz GS, Lin J, Valeri AM, D'AGATI. Glomerular tip lesion: a distinct entity within the minimal change disease/focal segmental glomerulosclerosis spectrum. Kidney international. 2004;65(5):1690-1702.
Thomas DB, Franceschini N, Hogan SL, Ten Holder S, Jennette CE, Falk RJ, Jennette JC. Clinical and pathologic characteristics of focal segmental glomerulosclerosis pathologic variants. Kidney international.2006;69(5):920-926.
Arias LF, Jiménez CA, Arroyave MJ. Histologic variants of primary focal segmental glomerulosclerosis: presentation and outcome. Jornal Brasileiro de Nefrologia.2013; 35(2):112-119.
Shakeel S, Mubarak M, Kazi JI. Frequency and clinic-pathological correlations of histopathological variants of pediatric idiopathic focal segmental glomerulosclerosis. Indian Journal of Nephrology. 2014;24(3):148.
Taneda S, Honda K, Uchida K, Nitta K, Yumura W, Oda H, Nagata M. Histological heterogeneity of glomerular segmental lesions in focal segmental glomerulosclerosis. International urology and nephrology.2012; 44(1):183-196.
D’Agati VD, Alster JM, Jennette JC, Thomas DB, Pullman J et al. Association of Histologic Variants in FSGS Clinical Trial with Presenting Features and Outcomes. Clin J Am Soc Nephrol. 2012; doi: 10.2215/cjn.06100612
Usha, Kumar S, Singh RG, Tapas S, Prakash J, Garbyal RS. Mesangioproliferative glomerulonephritis: an important glomerulonephritis in nephrotic syndrome of young adult. Indian J Pathol Microbiol.2008; 51:337–341
Waldherr R, Gubler ME, Levy M, Broyer M, Habib R. The significance of pure diffuse mesangial proliferation in idiopathic nephrotic syndrome. Clin Nephrol 1978;10:171-9.
Floege J, Eng E, Yound BA, Couser WG, Johnson RJ. Heparin suppresses mesangial cell proliferation and matrix expansion in experimental glomerulonephritis. Kidney Int 1993;43:369-80.
Gubler MC, Waldherr R, Levy M, et al. Idiopathic nephrotic syndrome with focal and segmental sclerosis and/or hyalinosis: Clinical course response to therapy, and long-term outcome. In: Strauss J, ed. Nephrotic Syndrome: Current Concepts in Diagnosis and Management. New York: Garland, 1979:193.
Gephardt GN, Tubbs RR, Popowniak KL, McMahon JT. Focal and segmental glomerulosclerosis: Immunohistologic study of 20 renal biopsy specimens. Arch Pathol Lab Med 1986;110:902.
Magil AB: Focal and segmental glomerulosclerosis. Mod Pathol 1991; 4:383-391.
Mongeau JG, Robitaille PO, Glermont MJ, Merovani A, Russo P: Focal segmental glomerulosclerosis (FSG) 20 years later. From toddler to grown-up. Clin Nephrol. 1993; 40:1-6.
Nachmann PH, Jennett JC, Folk RJ: In Brenner and Rector’s: The kidney. Tal MW, Yu ASL, Chertow. 9th edition,Elsevier Saundus. 2012, 1111-1121.
D’Agati VD, Fogo A B, Bruijn JA, Jennette JC. Pathologic classification of focal segmental glomerulosclerosis: a working proposal.American journal of kidney diseases. 2004; 43(2):368-382.
Rennke H, Klein PS. Pathogenesis and significance of non primary focal and segmental glomerulosclerosis. Am J Kidney Dis 1989;13:443-55.
Franceschini N, North KE, Kopp J B, Mckenzie L, Winkler C. NPHS2 gene, nephrotic syndrome and focal segmental glomerulosclerosis: a HuGE review. Genetics in Medicine. 2006;8(2):63-75.
Koziell A, Grech V, Hussain S, Lee G, Lenkkeri U, Tryggvason K, Scambler P. Genotype/phenotype correlations of NPHS1 and NPHS2 mutations in nephrotic syndrome advocate a functional inter-relationship in glomerular filtration. Human Molecular Genetics.2002;11(4):379-388.
Weins A, Kenlan P, HerbertS, Le TC, Villegas I, Kaplan B S, Pollak M R. Mutational and biological analysis of α-actinin-4 in focal segmental glomerulosclerosis. Journal of the American Society of Nephrology.2005;16(12):3694-3701.
Winn MP, Conlon PJ, Lynn KL, Farrington MK, Creazzo T, Hawkins AF, Rosenberg PB. A mutation in the TRPC6 cation channel causes familial focal segmental glomerulosclerosis. Science. 2005;308:1801-1804.
Pollak MR. The genetic basis of FSGS and steroid-resistant nephrosis. In Seminars in nephrology. 2003; (Vol. 23, No. 2, pp. 141-146). WB Saunders.
Reiser J, Polu KR, Moller CC, Kenlan P, Altintas MM, Wei C, Pollak MR. TRPC6 is a glomerular slit diaphragm-associated channel required for normal renal function. Nature genetics,2005; 37: 739-44.
Hinkes B, Wiggins RC, Gbadegesin R, Vlangos CN, Seelow D, Nurnberg G, Hildebrandt F. Positional cloning uncovers mutations in PLCE1 responsible for a nephrotic syndrome variant that may be reversible. Nature genetics. 2006;38(12):1397-1405.
Diomedi-Camassei F, Di Giandomenico S, Santorelli FM, Caridi G, Piemonte F, Montini G, Emma, F. COQ2 nephropathy: a newly described inherited mitochondriopathy with primary renal involvement. Journal of the American Society of Nephrology. 2007;18(10): 2773-2780.
D'Agati V. Pathologic classification of focal segmental glomerulosclerosis. In Seminars in nephrology. 2003; (Vol. 23, No. 2, pp. 117-134). WB Saunders.
Zollinger HU, Mihatsch MJ: Renal Pathology in Biopsy: Light, Electron and Immunofluorescent Microscopy and Clinical Aspects. 1st edition. Springer Verlag Berlin Heidelberg New York. 1978:8-17.
Ferrario F, Rastaldi MP, Pasi A. Secondary focal and segmental glomerulosclerosis, Nephrology Dialysis Transplantation. 1999;14(SUPPL. 3):58-67.
Nada R, Kharbanda JK, Bhatti A, Minz RW, Sakhuja V, Joshi K. Primary focal segmental glomerulosclerosis in adults: is the Indian cohort different?.Nephrology Dialysis Transplantation.2009; 24(12): 3701-3707.
Das P, Sharma A, Gupta R, Agarwal SK, Bagga A, Dinda AK. Histomorphological classification of focal segmental glomerulosclerosis: A critical evaluation of clinical, histologic and morphometric features. Saudi Journal of Kidney Diseases and Transplantation.2012; 23(5):1008.
Shi SF, Wang SX, Zhang YK, Zhao MH, Zou WZ.Clinicopathologic study of different variants of focal segmental glomerulosclerosis. Chinese journal of pathology. 2007;36(1):11-14.
Silverstein DM, Craver R. Presenting features and short-term outcome according to pathologic variant in childhood primary focal segmental glomerulosclerosis. Clinical Journal of the American Society of Nephrology, 2007; 2(4): 700-707.
Stokes MB, Markowitz GS, Lin J, Valeri AM, D'AGATI. Glomerular tip lesion: a distinct entity within the minimal change disease/focal segmental glomerulosclerosis spectrum. Kidney international. 2004;65(5):1690-1702.
Thomas DB, Franceschini N, Hogan SL, Ten Holder S, Jennette CE, Falk RJ, Jennette JC. Clinical and pathologic characteristics of focal segmental glomerulosclerosis pathologic variants. Kidney international.2006;69(5):920-926.
Arias LF, Jiménez CA, Arroyave MJ. Histologic variants of primary focal segmental glomerulosclerosis: presentation and outcome. Jornal Brasileiro de Nefrologia.2013; 35(2):112-119.
Shakeel S, Mubarak M, Kazi JI. Frequency and clinic-pathological correlations of histopathological variants of pediatric idiopathic focal segmental glomerulosclerosis. Indian Journal of Nephrology. 2014;24(3):148.
Taneda S, Honda K, Uchida K, Nitta K, Yumura W, Oda H, Nagata M. Histological heterogeneity of glomerular segmental lesions in focal segmental glomerulosclerosis. International urology and nephrology.2012; 44(1):183-196.
D’Agati VD, Alster JM, Jennette JC, Thomas DB, Pullman J et al. Association of Histologic Variants in FSGS Clinical Trial with Presenting Features and Outcomes. Clin J Am Soc Nephrol. 2012; doi: 10.2215/cjn.06100612
Usha, Kumar S, Singh RG, Tapas S, Prakash J, Garbyal RS. Mesangioproliferative glomerulonephritis: an important glomerulonephritis in nephrotic syndrome of young adult. Indian J Pathol Microbiol.2008; 51:337–341
Waldherr R, Gubler ME, Levy M, Broyer M, Habib R. The significance of pure diffuse mesangial proliferation in idiopathic nephrotic syndrome. Clin Nephrol 1978;10:171-9.
Floege J, Eng E, Yound BA, Couser WG, Johnson RJ. Heparin suppresses mesangial cell proliferation and matrix expansion in experimental glomerulonephritis. Kidney Int 1993;43:369-80.
Gubler MC, Waldherr R, Levy M, et al. Idiopathic nephrotic syndrome with focal and segmental sclerosis and/or hyalinosis: Clinical course response to therapy, and long-term outcome. In: Strauss J, ed. Nephrotic Syndrome: Current Concepts in Diagnosis and Management. New York: Garland, 1979:193.
Gephardt GN, Tubbs RR, Popowniak KL, McMahon JT. Focal and segmental glomerulosclerosis: Immunohistologic study of 20 renal biopsy specimens. Arch Pathol Lab Med 1986;110:902.
Published
2016-02-10
Issue
Section
Original Article
Authors who publish with this journal agree to the following terms:
- Authors retain copyright and grant the journal right of first publication with the work simultaneously licensed under a Creative Commons Attribution License that allows others to share the work with an acknowledgement of the work's authorship and initial publication in this journal.
- Authors are able to enter into separate, additional contractual arrangements for the non-exclusive distribution of the journal's published version of the work (e.g., post it to an institutional repository or publish it in a book), with an acknowledgement of its initial publication in this journal.
- Authors are permitted and encouraged to post their work online (e.g., in institutional repositories or on their website) prior to and during the submission process, as it can lead to productive exchanges, as well as earlier and greater citation of published work (See The Effect of Open Access at http://opcit.eprints.org/oacitation-biblio.html).

